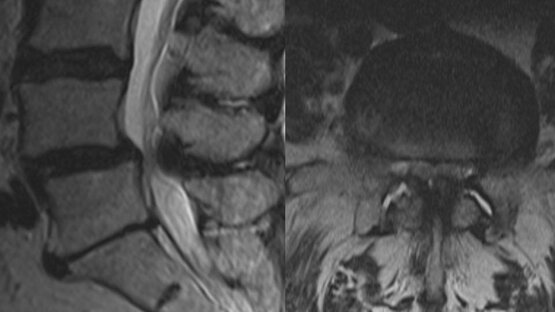
Disc herniation
Disc herniations are the main indication for the use of the VERTEBRIS system. The system was developed to address disc herniations that have failed treatment using more conservative therapies. The following objectives should always be a top priority of disc herniation surgery:
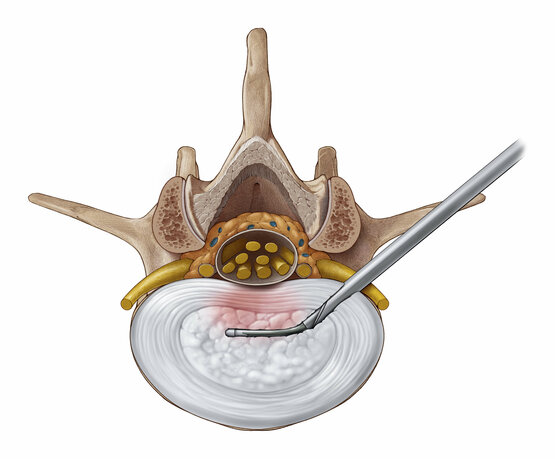
- Direct decompression of neural structures: using a "targeted approach" to access and remove the disc herniation by the most direct path possible.
- Most minimally invasive access: choosing the approach that minimizes trauma to the surrounding soft tissue and bone structures.
- Reducing the risk of recurrences: performing a partial and selective discectomy to reduce the risk of recurrences.
Standardized surgical approaches have been developed as part of the VERTEBRIS system to help ensure that the minimally invasive criteria is consistently maintained.
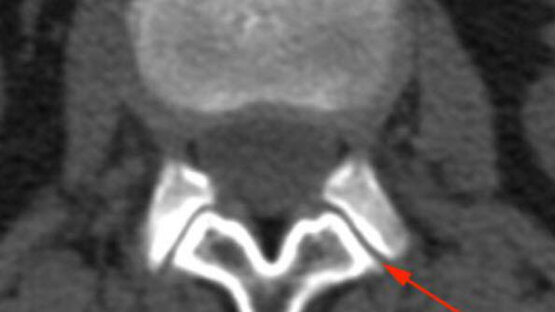
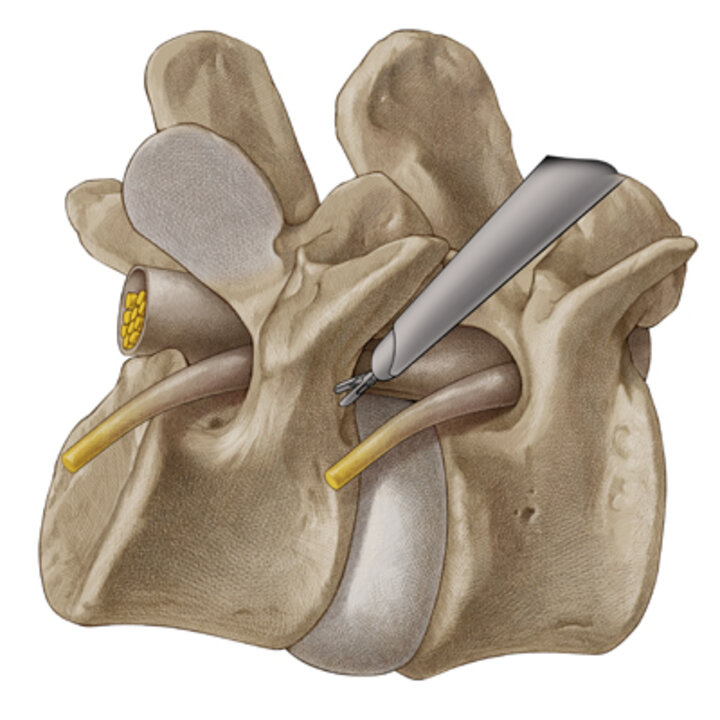
Transforaminal technique
The transforaminal technique involves positioning an access channel from a lateral to posterolateral approach with the tip targeting the intervertebral foramen to provide endoscopic access to the disc, epidural space and/or facets. While the transforaminal approach can be used for pathologies at all vertebral levels, it is most often used at L4/5 and higher segments.
In order to minimize the trauma of introducing the access channel, the approach should be tailored to the indications and specific location of the pathology:
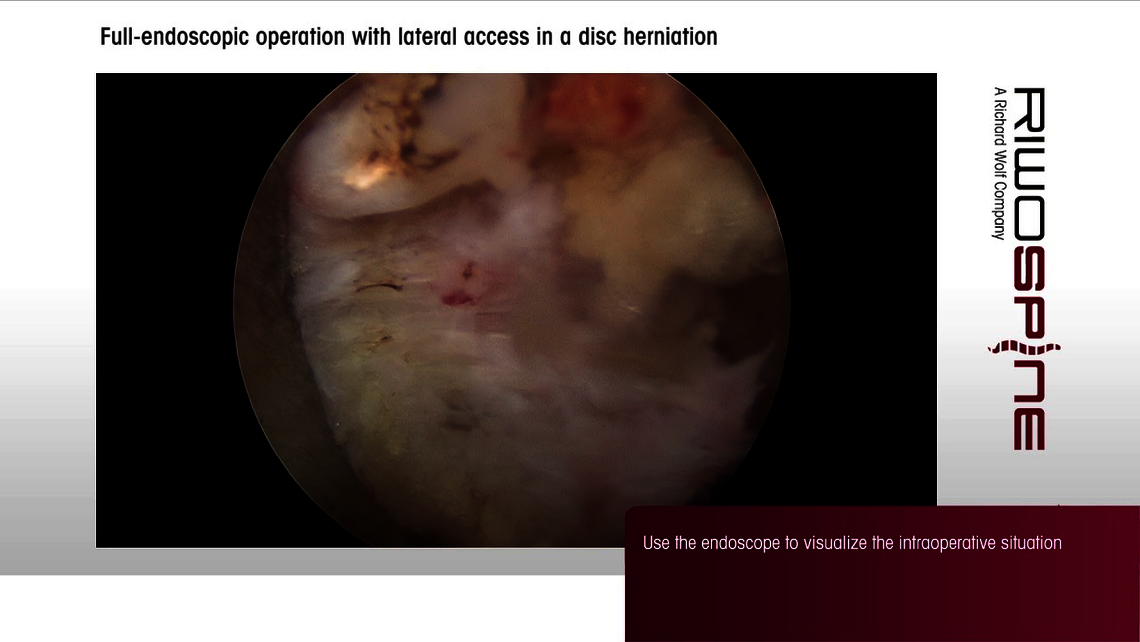
Lateral transforaminal approach
- Access direction approx. 20° to horizontal
- Used for intraspinal (mediolateral) and intraforaminal (lateral) localized pathologies
- Access to the ventral epidural space and the dorsal intervertebral disc
Posterolateral transforaminal approach
- Access direction approx. 45° to horizontal
- Used for intradiscally localized pathologies
- Access to the central disc
In narrow intervertebral foramina, parts of the ascending facet and pedicle can be removed with manual and motorized burrs to improve access.
Extraforaminal technique
The extraforaminal technique involves placing an access channel in a position similar to the transforaminal approach, but with the tip of the channel and endoscope initially positioned on a bony landmark outside of the foramen. This approach is preferred for extraforaminal disc herniations and for foraminal stenosis. It is useful at all segments of the lumbar and thoracic spine.
In the extraforaminal technique, the preferred access angle is 20° to 30° to the horizontal. In order to prevent injuries to the exiting nerve root, the tip of the working sleeve is anchored in the caudal pedicle. From there, the VERTEBRIS endoscope with working sleeve and instruments is moved cranially under full-endoscopic view to identify and remove herniated disc. Motorized burrs can be used under visualization to widen the foramen as necessary to improve access or relieve stenosis.
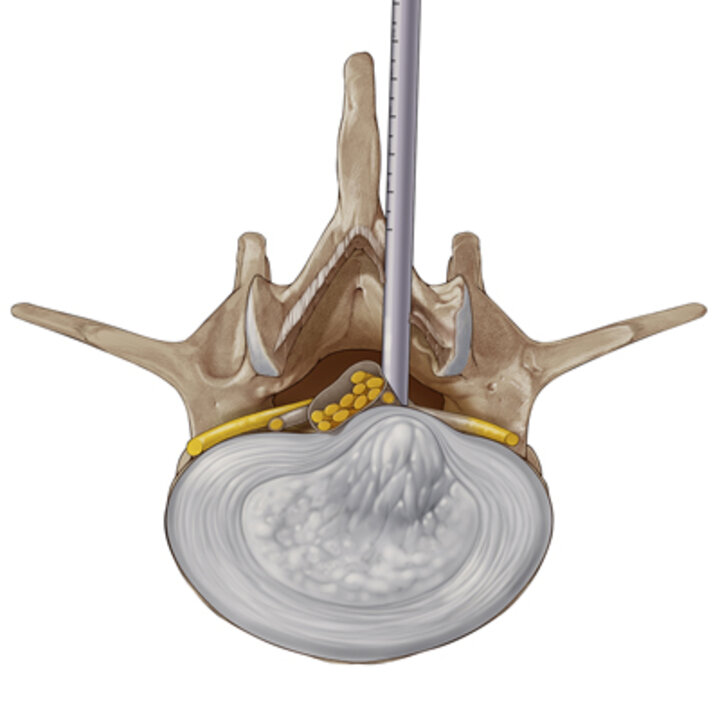
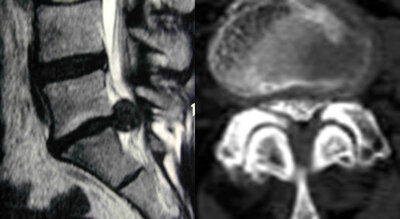
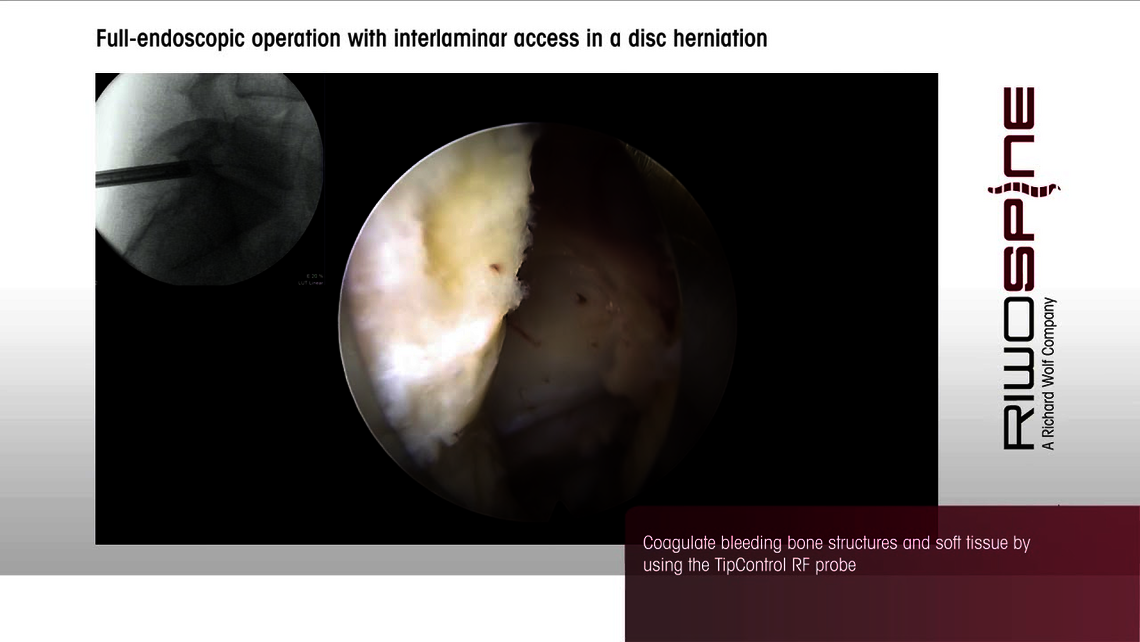
Interlaminar technique
In the interlaminar technique, a posterior approach is used to target the interlaminar window for access to the posterior disc and epidural space. Preferred indications for interlaminar access are intraspinal localized pathologies at the L5/S1 level and lateral recess stenosis and central canal stenosis.
The interlaminar window is usually large enough to accommodate the working sleeve at the L5/S1 level, so the use of burrs are generally not required at this level. However, if the interlaminar approach is used in higher segments of the spine, the use of a burr will likely be necessary to expand the interlaminar space in order to gain access to the epidural space. A burr will also be required if there is spinal stenosis that needs to be decompressed at that segment.
Cervical disc herniation

The main indications for endoscopic cervical operations are “soft” spinal disc herniations with radicular symptoms. The VERTEBRIS cervical full-endoscopic systems were developed to decompress the neural structures directly while minimizing the trauma in accessing them.
Two separate systems, one for an anterior approach and one for a posterior approach, were developed. To address the different anatomical requirements of the two approaches, each system has its own standardized surgical technique and unique instrumentation.
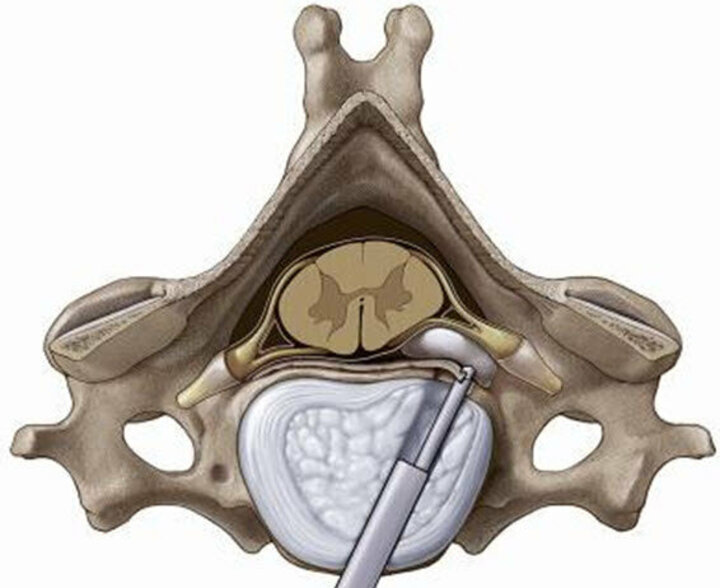
Anterior transdiscal surgical technique
The anterior cervical technique employs a working sleeve and special endoscope traversing obliquely through the disc space, from anterior to contralateral posterior. The indications for the endoscopic anterior approach are disc herniations located medially to mediolaterally, which cannot be reached with the posterior full-endoscopic approach.
After manual palpation and advancement past the ventral anatomical structures (esophagus, trachea, arteries), a thin dilator is inserted directly into the disk under x-ray control. A special oval dilation/sleeve system is pushed under X-ray view up to the dorsal edge of the cervical disk. After opening the dorsal annulus of the intervertebral discs and inserting the sleeve and endoscope, the herniated disc is removed transdiscally under endoscopic view.
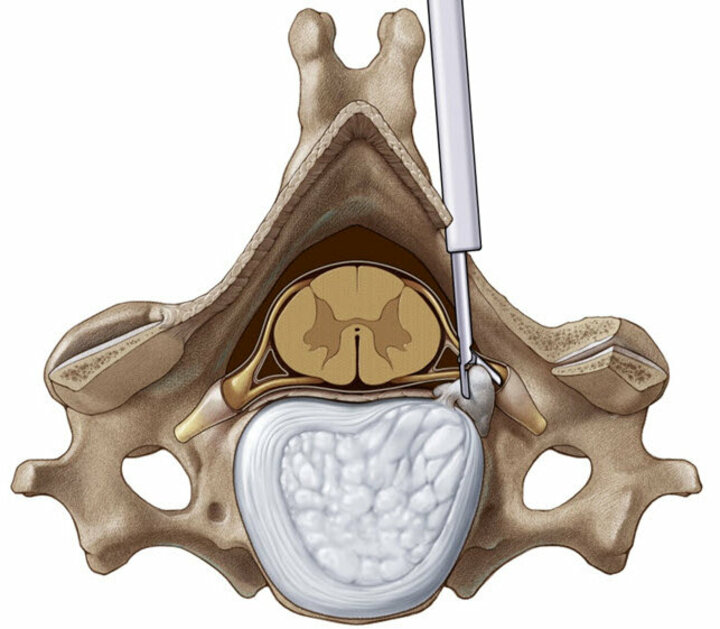
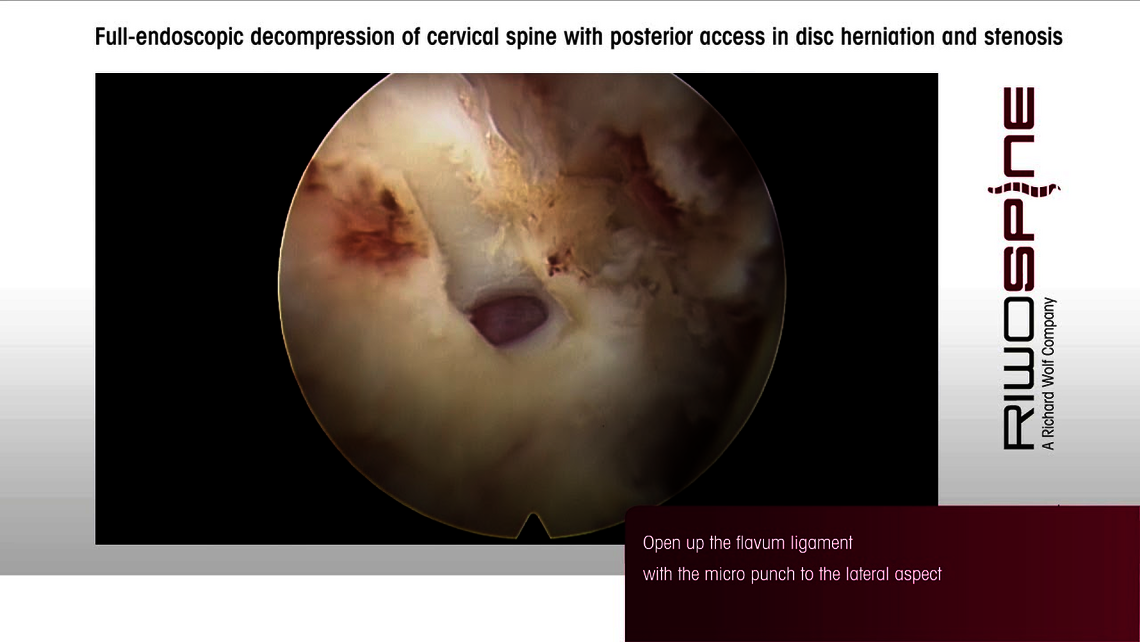
Posterior surgical technique
The posterior cervical approach is essentially an interlaminar approach applied to the cervical vertebrae. Indications for the full-endoscopic posterior approach are mainly mediolaterally to laterally localized herniated disks.
A 7 mm. diameter working sleeve allows for relatively atraumatic access through the soft tissue until the laminae and the facet joint are reached. Using high-resolution endoscopic visualization, parts of the laminae and the facet joint can be removed with mechanical burrs. The nerve root can then be identified and the disc herniated disc removed.

Pioneering endoscopic spine surgery
Richard Wolf / RIWOspine has long been the leader in pioneering full-endoscopic spine surgery with the development of specialized instrumentation and standardized techniques, combined with enabling technologies such as high resolution endoscopes, HD imaging systems, and articulating instruments.