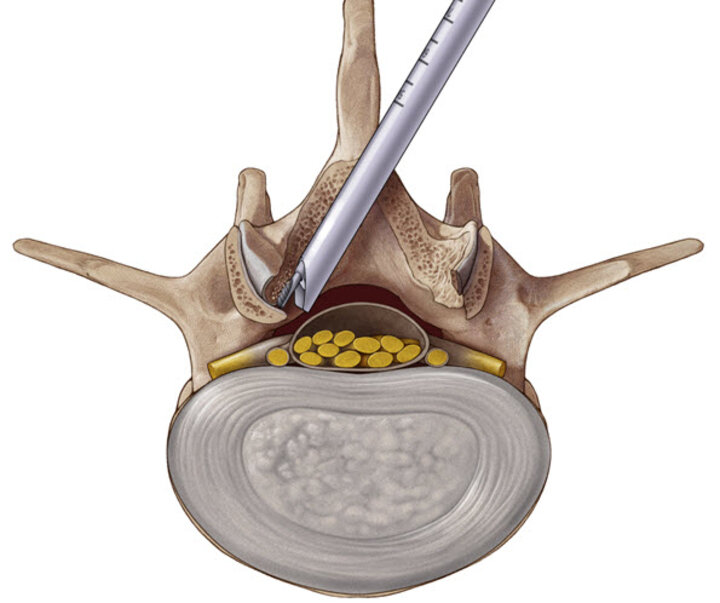
Spinal canal stenosis
Neural structures of the spine can become compressed by the bony and ligamentous tissues of the spinal canal. Stenosis can be categorized by localizing the constriction to the lateral structures (foraminal stenosis and lateral recess stenosis) or to the central canal (central stenosis)..
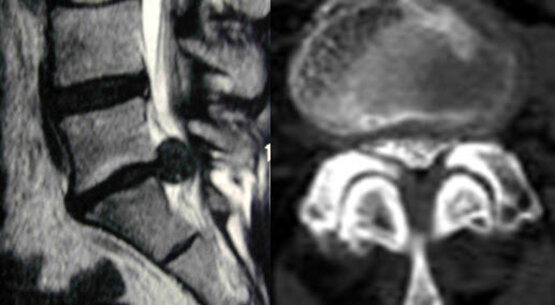
Foraminal stenosis
Stenosis of the foramen leads to compression of the exiting nerve root and manifests as primarily radicular symptoms. The cause of foraminal stenosis is degenerative bony structures at the facet joints and pedicles.
Surgical options:
1. The preferred method to address foraminal stenosis is to perform resection of the foraminal bone using a full-endoscopic transforaminal or extraforaminal approach. The Tip-Control Articulating Burr is used through the VERTEBRIS lumbar endoscopic system to remove the impinging bone under direct endoscopic visualization. Nearby neural structures are visually identified and protected with the working sleeve.
2. Alternatively, it is possible to use trephines or hand burrs percutaneously to widen the foramen. The instruments are positioned and used under fluoroscopic visualization.

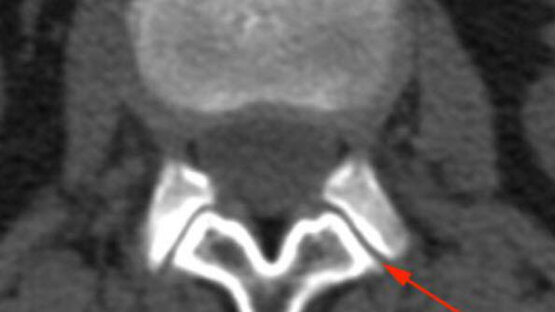
Lateral recess stenosis
Lateral recess stenosis causes compression of the traversing nerve root and lateral portions of the spinal cord. This is a result of constriction of the bony structures in the lateral recess of the spinal canal.
Surgical options:
Stenosis in the lateral recess can be addressed by careful resection of bone through a full-endoscopic interlaminar approach. A variety of burrs are available to remove the impinging bone through the VERTEBRIS lumbar endoscopic system under direct endoscopic visualization.
The approach is more lateral than the standard interlaminar approach. First, with the ligamentum flavum still intact, a burr is used to resect the descending articular process from its caudal tip up to the level of the tip of the ascending articular process. Next the ligamentum flavum is opened using suitable punches and the neural structures are localized before the lateral decompression of the facet is finished using diamond burrs or laterally hooded carbide burrs.
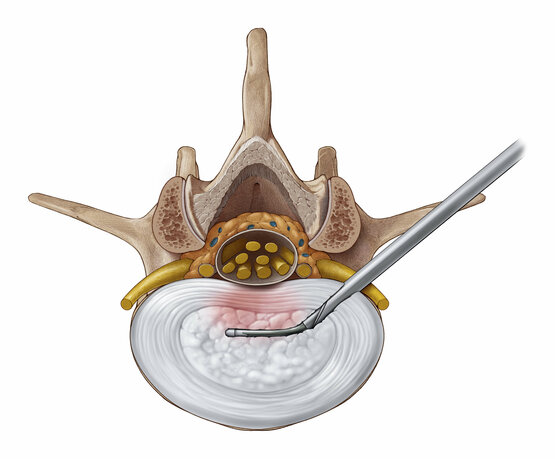
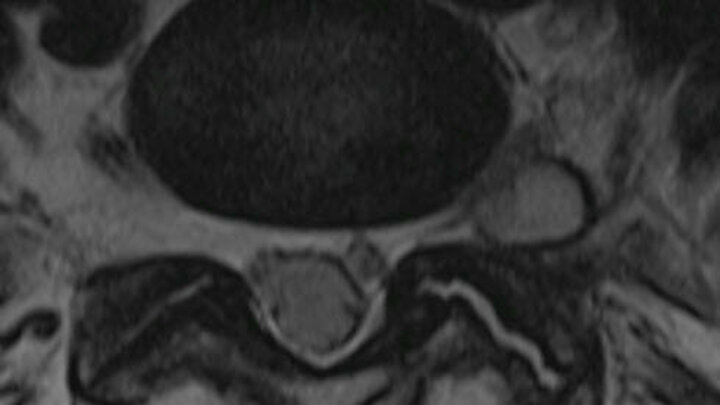
Central stenosis
Central stenosis may cause compression of lateral and central parts of the spinal cord as well as of traversing nerve roots depending on their location and characteristics. Correspondingly the patient’s symptoms may be central or radicular in nature.
Surgical options:
Central stenosis can be addressed by resection of the impinging bone and hypertrophied ligamentum flavum using an ipsilateral full-endoscopic interlaminar approach with additional extension of the procedure to the contralateral side.
The VERTEBRIS stenosis system was developed especially to perform bilateral bony decompression of the lumbar spine with the same effectiveness as conventional MIS and open procedures.
The procedure is started in the same manner as the recess stenosis case mentioned above. Additionally, the bone resection is extended towards the cranial and caudal lamina. Afterwards, the resection of the ligamentum flavum is carried towards the contralateral side with Kerrison punches. The decompression of the contralateral recess is performed with an “undercutting technique“ using special burrs (i.e., diamond and eccentric laterally protected burrs) to protect the neural structures.
Compared to conventional surgery, the full-endoscopic decompression can be done more selectively by sparing surrounding bone and tissue structures that do not affect the compression.

Ipsilateral decompression on one side
After the access has been created, the bony structures are exposed. Decompression typically starts at the caudal end of the descending facet. Depending on the pathology, decompression continues with resection of a portion of the medial descending facet, the cranial and caudal lamina, and the ligamentum flavum. The extent of decompression generally continues cranially at least until the tip of the ascending facet and caudally to half of the pedicle.
The medial portions of the ascending facet and the ligamentum flavum are then resected until sufficient decompression of the neural structures can be clearly seen - cranially, caudally and laterally. In the case of a central stenosis, the ligamentum flavum generally needs to be resected medially to the midline.
Finally, it may be necessary to remove protruding annulus and osteophytes in the ventral epidural space.

Contralateral decompression in over-the-top technique
If bilateral symptoms are present with central stenosis, a unilateral approach can be carried out with additional "over-the-top" access using the undercutting technique to reach the opposite side. For this purpose, bone in the ventral area of the spinous process is resected until the contralateral side can be accessed dorsally up to the dura of the spinal cord. If possible, the ligamentum flavum is initially left in place to protect the dura, and bony decompression is again carried out by laminotomy and partial facetectomy. The ligamentum flavum is then completely resected. Finally, the contralateral recess will likely need to be extended. The decompression is completed when the dura and the spinal nerves have been clearly decompressed.
An extended and uninterrupted excessive retraction of the neural structures with the working sleeve in a medial direction must be avoided particularly in cranial areas, or only carried out intermittently, in order to avoid the risk of neurological damage.


Pioneering endoscopic spine surgery
Richard Wolf / RIWOspine has long been the leader in pioneering full-endoscopic spine surgery with the development of specialized instrumentation and standardized techniques, combined with enabling technologies such as high resolution endoscopes, HD imaging systems, and articulating instruments.